Hall ticket no :16010016057 , long case
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome."
I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
CASE:
A 14 year old male resident of nalgonda , student by occupation,came to opd three days back with Chief complaints of
Cough since 8 days
and shortness of breath since 8 days
Fever since 8 days
History of present illness :
Patient was apparently asymptomatic
8 days ago
And then he developed fever - insidious onset ,Low grade continuous a/s with chills and rigors relieved on medication
H/o SOB Since 8 days insidious onset
Progressive from MMRC 1 to 2nd
Increased on exertion and cough
Relieved on sitting position,no diurrnal , positional variation
(No orthopnea and PND)
H/o of dry Cough - since 8 days , insidious onset,non progressive ,no aggravating and relieving factors,no positional variation
Loss of appetite
No complains of chest pain
Burning micturition
Loss of weight
No hlo of tb
PAST HISTORY:H/o of similar complaints since5-6 years ( on regular inhaler usage )(asthalin,bordecort)
no history of TB ,diabetes mellitus , epilepsy, hypertension
PERSONAL HISTORY:
Appetite:decreased appetite
Diet: mixed
B and b - regular
Sleep - adequate
No addictions
FAMILY HISTORY:no history of similar complaints in family
GENERAL EXAMINATION:
Patient is consious, coherent,cooperative,oreinted to time ,place , person comfortably lying on bed
Moderately built and nourished
Pallor absent
No signs of
Cyanosis
Clubbing
Koilonychia
Generalized lymphadenopathy
VITALS:pulse : 90 beats per minute
Blood pressure:110/70 mmhg on supine position
Respiratory system-18 cycles per min
Temperature: afebrile
Spo2-95%
LOCAL EXAMINATION OF respiratory system
Inspection:
Shape of chest - elliptical , bilateral symmetrical
No deformity
Trachea position:central , expansion of chest decreased on left side
Apical impulse couldn't be seen
No use of accessory muscles of respiration
No Supra or infra clavicular hollowness or fullness
No drooping of shoulder
No .crowding of ribs
No wasting of muscles
No scars ,sinuses,dialted veins in thorax region
Spinaspaculular distanced is increased on left side
PALPATION:No local rise in temperature and tenderness
All inspectory findings confirmed by palpation
No local rise of. Temperature
Trachea : central
Chest movements decreased on left side
Apex beat:left 5th intercoastalspace 1cm to the medial to MCL
TVF -decreased on left infra scapular ,IAA,AA ,
Percussion:
Direct: resonant
Indirect -dull on left infra SA and inter SA
AA;IAA
Auscultation:
Bilateral air entry : positive
Decreased breath sounds - ISA,IAA,interscapular area
Added sounds: absent
CVS system :
S1
S2 present
No murmurs
Per abdomen : soft,non tender,no organomegaly
CNS EXAMINATION: intact
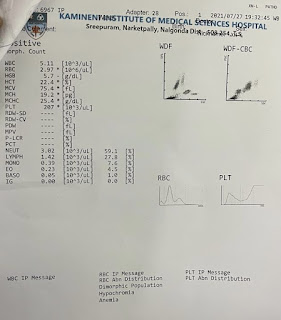
INVESTIGATIONS:
Haemogram :slight decrease in haemoglobin

Chest X ray:

Thoracocentesis-
Pleural fluid: sugar and protein normal




Serum electrolytes: chloride is increased

Liver function test:t
Total bilirubin and direct bilirubin increased
SGPT (ALT) - normal
ALP- normal
SGOT(AST) -normal




ECG


Serum protein is decreased




Treatment: conservative treatment
1:
Cefixime 200mg bd
Azithromycin 500 mg od
Tablet pantoprazole
40 mg od
(Nebulizer with asthalin 6th hourly)
Budecort 8th hourly
Montac - OD


Comments
Post a Comment