G.Preethi , 1601006057, roll no :50
56Y old female came to OP with chief complaints of
fever since 1 month
B/L swelling of lower limb since 1month
Loss of apetite since 20 day
Generalised weaknesa since 20 days
Vomitings since 3 daysdays
History of present illness :
- Fever was high grade, intermittent not associated with chills and rigors , cold and cough.
- Associated with decreased apetite and generalised weakness, burning micturation was on and off and associated with suprapubic pain
- Swelling of lower limbs was on and off since 2 years and not associated with SOB, palpatations, decreased urine output, facial puffiness
- on presentation pedal edema was not seen.
patient denied the history of usage of Nsaids . Patient was apparently asymptomatic 10 yrs back had severe menstrual flow , consulted a gynaecologist . She was advised for hysterectomy-operated and biopsy was done .
- History of past illness : after 6 months(2012) of hysterectomy on general follow up she was diagnosed as DM-2 and on tab -metformin (500mg po/od Patient was on regular medication. Intermittent tingling sensation of B/L LL+.
Treatment history :
diabetic-10 yrs .
Metformin 500mg po/od
Surgeries - hysterectomy.
-Personal history : Married
Occupation:daily labourer.
Appetite:lost (20yrs)
Diet :non vegetarian.
Bowels :regular
Bladder : abnormal (burning micrurition ( intermittent)
Habits : alcohol - no
Tobacco-no.
Drug uses - no
Family history- not relevant.
Menstrual history :
Age of menarchae -12 yrs
Obstetric history -
Age at marriage - 14 yrs
Age at first child birth. - 16 yrs.
gravida - 5 ,para -5 ,
Still birth :- no , no of living children :5 No abortions
Birth history : FTND , no history of birth asphyxia. Developmental history-normal.
Physical examination :
General :
Pallor :++.
Icterus :no.
Cyanosis :no.
Clubbing :no.
Lymphadenopathy:no.
Oedema of feet : no.
Malnutrition: no.
Dehydration: no.
Temperature:afebrile
PR:106bpm.
RR:18cpm.
BP:110/80mm Hg.
Spo2: at room air -96%.
GRBS -166mg%.
Systemic examination:
CVS : s1, s2 heard
Respiratory system :
BAE +
trachea central in position
NVBS +
Abdomen : normal.
CNS : NAD
Provisional diagnosis
AKI on CKD with k/c/o DM-2 since 10 yrs with anemia under evaluation.
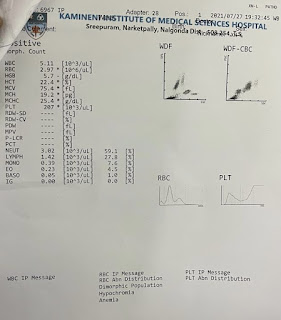
Investigations :
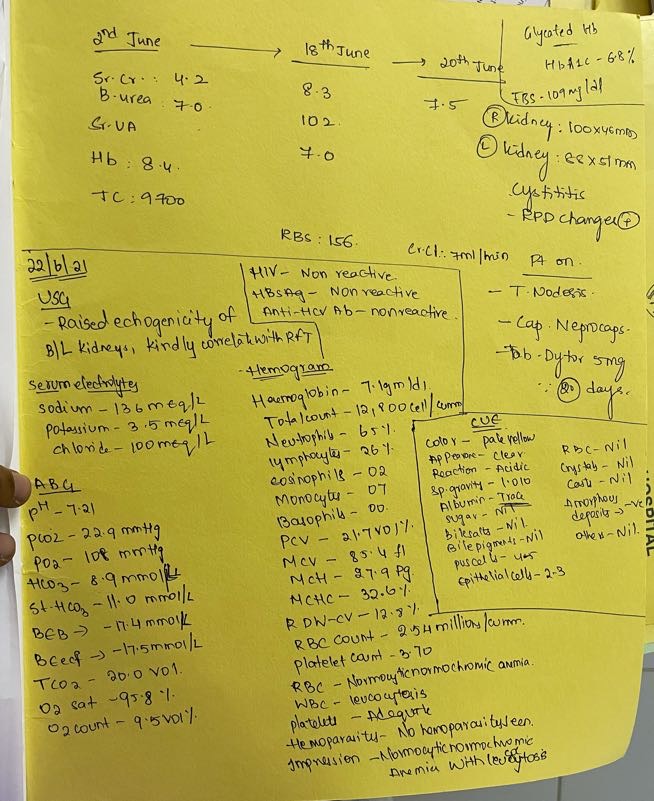
USG :

RBS :

Serum creatinine:(22/6/21)

FBS:

HBA1c:

Serum creatinine (23/6/21):


ECG :

Urine protein /creatine ratio (24 /6)

Serum creatinine (25/6)

Blood urea ( 25/6)

Serum electrolytes (25/6 )

ABG :

Urine culture

Sputum culture :

Treatment :
Day -1
Vitals :
Temperature:98.6•F
PR:102bpm
Bp :110/60mm hg
GRBS : 176mg/dl
IVF - uo +30 ml /hr
Tab Lasix
Tab :orofer
Tab :nodosis
Inj : HAI s/c acc to sliding scale
GRBS charting
Day :2
Vitals :
Temperature: a febrile
PR : 108bpm
BP:120/70mmhg
GRBS :176mg/dl
Ivf-uo +30 ml/hr
Inj pantop
Inj zofer
Inj :Lasix
Tab :orofer
Tab :nodosis


Comments
Post a Comment